About the Study
The Canadian Alliance for Healthy Hearts and Minds (CAHHM) study is a multicenter cohort study that recruited participants from existing Canadian cohort studies between 2014-2018. All participants underwent an assessment of cardiovascular health, imaging biomarkers (including MRI of the brain, heart, carotid arteries, and adipose tissue), and social factors. Study participants provided permission for record linkage using their health card number, allowing for ongoing prospective follow up both regionally and nationally.
CAHHM is a deeply phenotyped, innovative cohort study with deliberate recruitment of diverse populations. For example, the study includes 60% female participants and a significant proportion of Chinese, South Asian, and Black Canadians.
Starting in late 2023, the CAHHM study initiated recontact of select CAHHM participants involving a two-phase follow-up, with Phase 1 updating participants’ health status via online questionnaires and Phase 2 inviting eligible participants for repeat MRI and clinical assessments. The overarching goal is to delineate the pathways connecting EAT to cognitive decline, considering pre-clinical vascular disease, biomarkers, and lifestyle factors.
All participants underwent an assessment of cardiovascular health, imaging biomarkers (including MRI of the brain, heart, carotid arteries, and adipose tissue), and social factors. Study participants provided permission for record linkage using their health card number, allowing for ongoing prospective follow up both regionally and nationally.
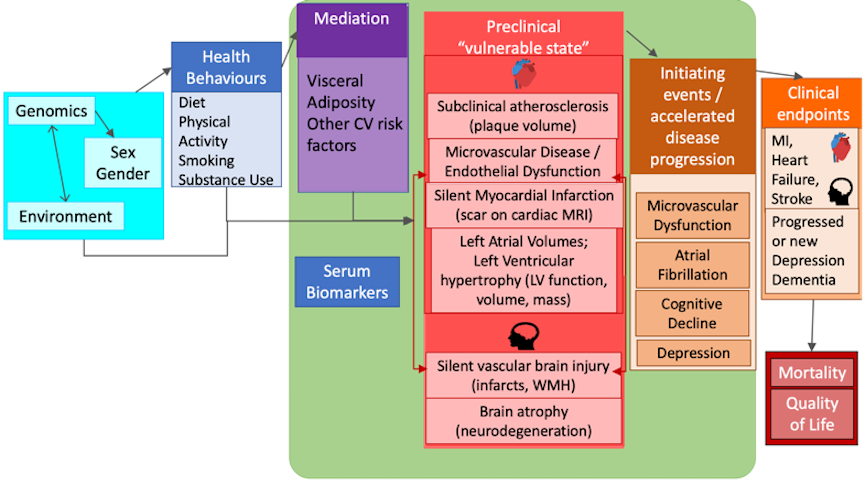
Pathways to Healthy Hearts and Minds Framework
Additional information about the study is available in the July 2016 design paper published in BMC Public Health.
Pathways to Healthy Hearts and Minds Framework
Additional information about the study is available in the July 2016 design paper published in BMC Public Health.
CAHHM initially consented 10,100 participants across Canada. Of these participants, 8,580 consented to participate in the full study; while the remaining 1,520 solely completed the Health Services Research questionnaire.
Participants across Canada
N=10,100
Services Research questionnaire
N=1,520
N=8,580
N=8,258
Participants in the full study underwent detailed cerebrovascular, cardiac, and cognitive phenotyping. Furthermore, detailed information on health behaviours (diet by food frequency questionnaire, physical activity using the IPAQ, substance use), access to healthcare, and community audits of the built environment were collected. MRI of the heart, brain, carotid arteries, and abdomen were completed on N=8,258 (96.2%) participants.
CAHHM is a national “cohort of cohorts” which recruited participants already enrolled in existing Canadian cohort studies. The full study included participants from the Canadian Partnership for Tomorrow’s Health (CanPath) n=6,522, Prospective Urban Rural Evaluation (PURE) n=1133, Montreal Heart Institute BioBank n=360, and a new Chinese-Canadian cohort in Toronto, ON (n=565).
Information collected
Blood pressure, heart rate, waist and hip circumference, height, weight, and percentage body fat. View the physical measurements questionnaire.
The Montreal Cognitive Assessment (MoCA) is a cognitive screening test designed to assist Health Professionals in the detection of mild cognitive impairment and Alzheimer’s disease. Click here to view the published validation, and click here to view the MoCA questionnaire. The Digital Symbol Substitution Test (DSST) is a subtest of the WAIS-IV cognitive screening test designed to measure cognitive impairment. View the DDST.
The International Physical Activity Questionnaire (IPAQ) assesses energy expenditure by tracking daily exertion. The long IPAQ was collected in about 40% of participants, and the short IPAQ was collected in about 60% of participants. Click here to view a systematic review validating the use of the IPAQ. View the physical activity questionnaire.
The INTERHEART Risk Score questionnaire is a validated score that factors in data on age, sex, smoking status, diabetes, high blood pressure, family history of heart disease, waist-to-hip ratio, psychosocial factors, diet and physical activity. Click here to view a recent INTERHEART Risk Score validity publication, and click here to view the INTERHEART risk score questionnaire.
The Health Services Research and Cardiovascular Questionnaire (HSR) examines participants’ access to health care services, such as visits to a primary care provider or the emergency department, or language barriers affecting care provision. The questionnaire also collects information focused on cardiovascular risk factors, history of cardiovascular diseases, and medication use. View the HSR questionnaire.
Social capital data was collected via the CAHHM Community Contextual Factors Questionnaire, which was replicated from the Environmental Profile of Community Health (EPOCH-2) instrument that has been studied and validated in five countries, including Canada (Anand et al., 2018b; Chow et al., 2010; Corsi et al., 2012). The questionnaire assesses the individual contextual factors in the built environment of participants in the study that may have an impact on health, such as: community advertising related to smoking/tobacco, food, alcohol, and physical activity; community environments related to tobacco, alcohol, nutrition/physical activity, and socializing; relationships with family and friends; civic engagement; life satisfaction; individual home and workplace environment. View the contextual factors assessment questionnaire.
The immigration questionnaire assesses the sense of cultural belonging and connection amongst immigrant participants enrolled in the study. View the immigration questionnaire, the acculturation questionnaire, and the Vancouver index of acculturation questionnaire.
The Canadian Partnership for Tomorrow’s Project questionnaire. View the CPTP questionnaire.
Dietary assessment tool capturing the amount and frequency of food intake and nutrient intake designed for white/Europeans, Chinese, and South Asians. View the white/European FFQ, Chinese FFQ, and South Asians FFQ.
Magnetic resonance imaging (MRI) of the brain, heart, carotid artery and abdomen.
A list of past patient medical history including documentation of medication use.
A cardiovascular MRI
study of the CAHHM cohort
A cardiovascular MRI study of the CAHHM cohort
At the beginning of 2022, a paper for CMR-derived sex and age-stratified normal references for ventricular and left atrial parameters was published in the JCMR by Luu et al (Luu et al. J Cardiovasc Magn Reson. 2022;24: 1–13.).
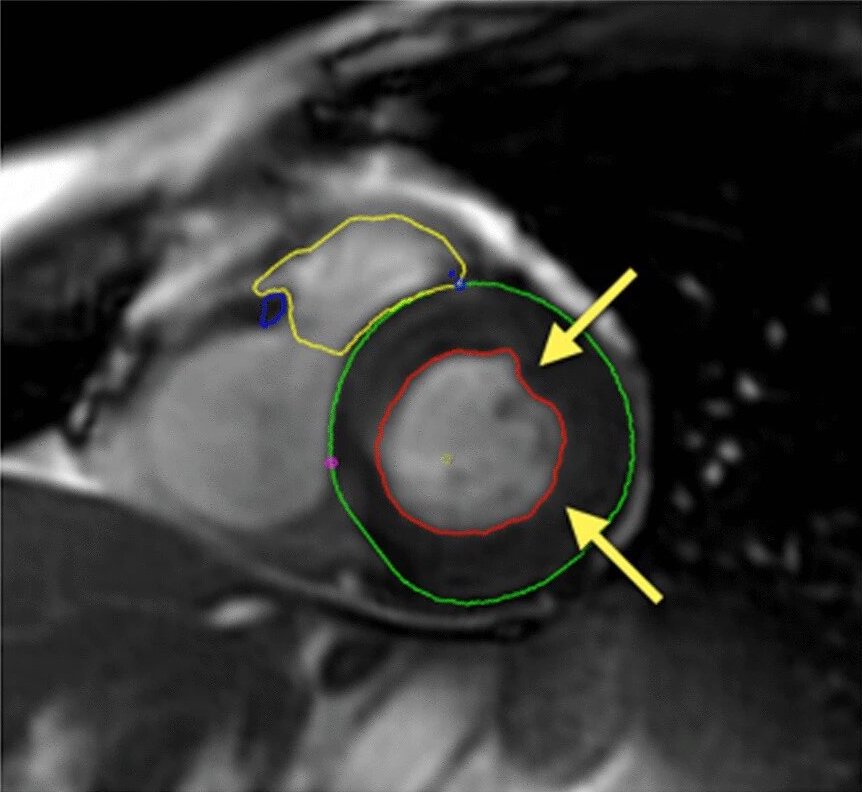
The paper stands out in several ways. It has the largest multi-ethnic reference population (> 3,000 participants) without cardiovascular disease or CV risk factors to date, and it provides definitive data because the researchers used anatomically correct contouring, incorporating papillary muscles and trabeculations as part of LV mass (Figure 1), with emphasis on defining LV mass at end-systole (Figure 2). The data are also reported separately (supplementary material) for white Caucasian, Chinese, and South Asian race/ethnicities, as well as indexed to BSA and height.
The 8-year project was performed as a sub-study of the Canadian Alliance for Healthy Hearts and Minds cohort, so the CMR data including contextual data are accessible for researchers.
Figure 1
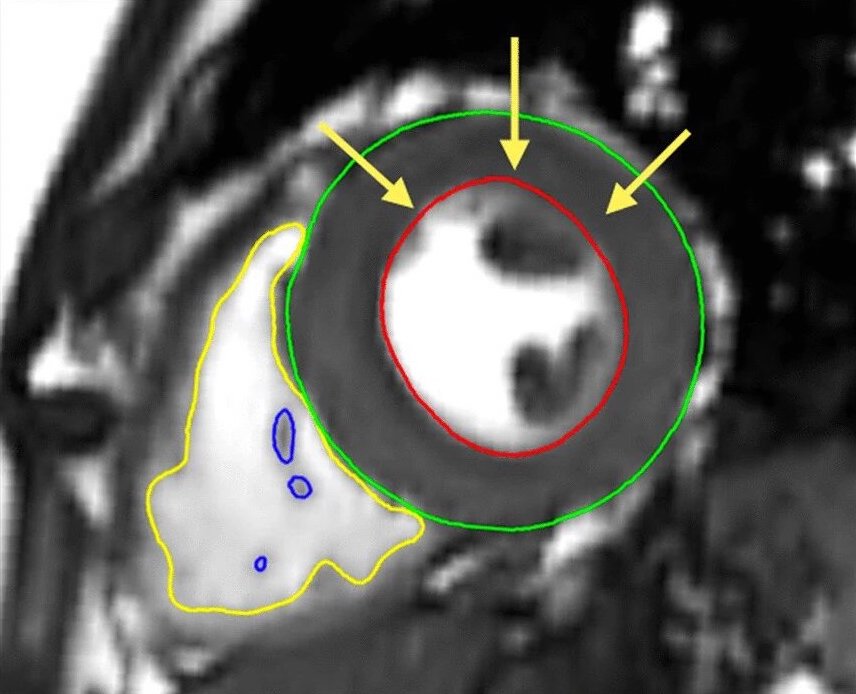
Simplified method
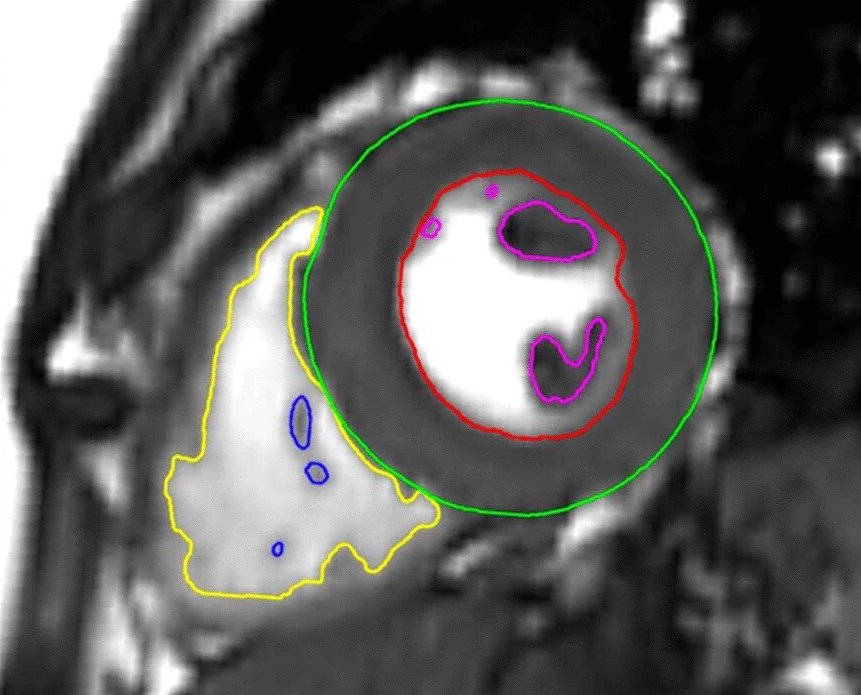
Anatomically correct method
Figure 2
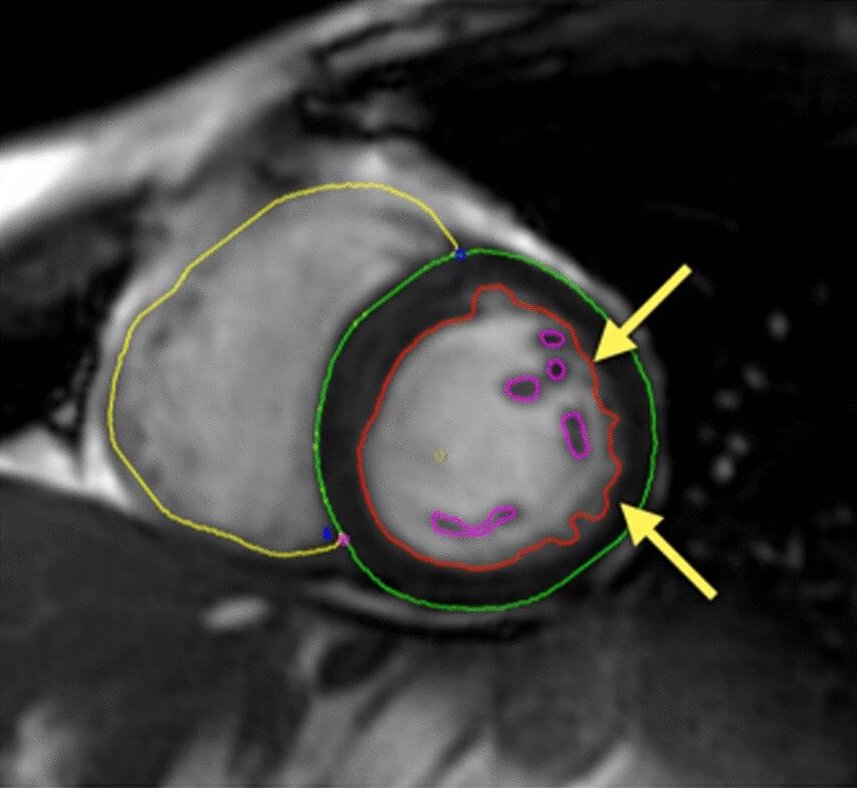
Irregular surface and contour because of trabeculations during diastole (first image) are less pronounced during systole (second image)
Irregular surface and contour because of trabeculations during diastole (left) are less pronounced during systole (right)